I came across a couple of resources and started to appreciate how different fructose is from glucose. In the low carb community, carbohydrates are obviously avoided or at least high amounts of it as they are generally considered bad. I support this approach but when we zoom in on fructose we notice that it is not so much glucose that is causing all typical chronic diseases but fructose.
Sugar is associated with metabolic syndrome (hypertension, insulin resistance, Type 2 Diabetes, NAFLD, cancer, …) as well as brain-related issues such as Alzheimer’s, dementia, Parkinson etc.. but what is it about sugar that makes us succumb to disease? Being half glucose half fructose, there are only 2 components to look into.
Can it really be glucose? We do have populations that have been eating high amounts of rice, wheat, potatoes… products that are all high in starch which get broken down into glucose and absorbed into our body. Yet metabolic syndrome is something that started to appear and evolved since the 1900’s.
What I will show you here is how fructose is causal to a lot of these diseases so that you understand it is fructose specifically that needs to be kept out of the diet. I do not recommend high starchy foods (glucose) either due to other factors but that is not the focus of this article.
Immediately some people will reflect on fruit because that is what we usually associate with fructose. The danger from fructose comes from a combination of quantity and speed so there is less to worry about as most fruit comes in a package of fiber that needs to be munched down so that speed and quantity is low. However, if you take down for example 3 or 4 oranges in one go then you’re no better off than drinking a glass of sugar sweetened beverage (SSB).
As a starter I would advice to listen to the Attia podcast with Rick Johnson, M.D. , researcher of fructose since many years. The podcast is packed with knowledge, it has opened my mind on fructose. I’ve used it to find research papers to support the link with the diseases I’m listing below.
Insulin Resistance (IR)
A first topic I already covered in another article where I explain about the differences in Insulin Resistance based on fructose versus low carb. It comes down to fructose metabolism causing a buildup of diacylglycerol or DAG. The effect of it is that it prevents insulin signaling.
To show you that the effect of fructose is real and already known since a long time. The paper below tested a hypocaloric diet with different liquid forms (glucose, galactose and fructose) in 14 days. They discuss other papers where they have seen every time that hypocaloric diets increase the insulin receptor in different cell types. This is an effect attributed to the hypocaloric content. What they noted was that in case of fructose there was no such increase in insulin receptors.
“Comparative effects of several simple carbohydrates on erythrocyte insulin receptors in obese subjects.” https://www.ncbi.nlm.nih.gov/pubmed/3534894
IR leads to Type 2 Diabetes Melitus (T2DM). A very recent paper shows us there is a dose response effect between the serum fructose levels and risk of T2DM.
“Fasting Serum Fructose Levels Are Associated With Risk of Incident Type 2 Diabetes in Middle-Aged and Older Chinese Population” https://pubmed.ncbi.nlm.nih.gov/32611608/
Non-Alcoholic Fatty Liver Disease (NAFLD)
Closely linked to IR we have NAFLD. The accumulating fat from the fructose metabolism in the liver causes IR but if it further aggravates then it develops into NAFLD.
There is a specific mechanism activated in response to the high fructose availability and that is carbohydrate response element–binding protein (ChREBP). This mechanism increases cholesterol synthesis but it also stimulates de novo lipogenesis. That is unfortunate because it is the buildup of fat that is causing the problems so creating more fat is the last thing needed.
ChREBP is specifically responsive to fructose.
“Lipogenic transcription factor ChREBP mediates fructose-induced metabolic adaptations to prevent hepatotoxicity” https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5490767/
Commentary: “ChREBP refines the hepatic response to fructose to protect the liver from injury” https://www.jci.org/articles/view/95008
I suspect that fructose has a similar profile to glucose to stimulate ChREBP. This is how excess in glucose is handled. There is a second pathway via SREBP1c but this is insulin mediated. ChREBP downregulates SREBP2 yet in how far that is different from SREBP1 is unknown to me at the moment. It is possible that with IR already build up, insulin won’t be able to activate SREBP1 much.
What is important here is that when de novo lipogenesis is activated, it also converts glucose to fat. So not only does fructose get turned into fat in the liver, it also stimulates the conversion of glucose to fat in the liver.
“De novo lipogenesis in the liver in health and disease: more than just a shunting yard for glucose” https://onlinelibrary.wiley.com/doi/full/10.1111/brv.12178
Visceral fat
The fat that is stored in the organs is visceral fat. This is unhealthy versus when it is stored underneath the skin where it is supposed to be stored.
For reasons that are still unknown although a link is suspected with the brain, fructose causes preferentially visceral fat storage. This doesn’t happen with glucose.
“Consuming fructose-sweetened, not glucose-sweetened, beverages increases visceral adiposity and lipids and decreases insulin sensitivity in overweight/obese humans.” https://www.ncbi.nlm.nih.gov/pubmed/19381015?dopt=Abstract
“Sucrose-sweetened beverages increase fat storage in the liver, muscle, and visceral fat depot: a 6-mo randomized intervention study” https://academic.oup.com/ajcn/article/95/2/283/4576708?ijkey=dd5aa94b6d0cdeaf811c029cac4234a839f07905&keytype2=tf_ipsecsha
Brain decline
Glucose and fructose have differential effect on the brain apart from the regions where there is overlap. What is interesting to see is that fructose causes a reduction in blood flow in the region that is affected by Alzheimer’s disease.
Hippocampal atrophy is part of Alzheimer’s disease. What does fructose do in a mouse study? Likely as a result of the reduced blood flow it could cause hypoxia and of course the hypoperfusion leading to insufficient nutrition with atrophy as a consequence.
Fructose consumption reduced the levels of the neuronal nuclear protein NeuN, Myelin Basic Protein, and the axonal growth-associated protein 43, concomitant with a decline in hippocampal weight.
“Acute Effects of Glucose and Fructose Administration on the Neural Correlates of Cognitive Functioning in Healthy Subjects: A Pilot Study” https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5857887/
“Pathology and hippocampal atrophy in Alzheimer’s disease” https://www.thelancet.com/journals/laneur/article/PIIS1474-4422(17)30343-5/fulltext
“Short-term fructose ingestion affects the brain independently from establishment of metabolic syndrome” https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5705281/
“Effects of Fructose vs Glucose on Regional Cerebral Blood Flow in Brain Regions Involved With Appetite and Reward Pathways” https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4076145/
The ApoE4 allele is particularily impacted by hypoxia resulting in reduced clearance of the beta-amyloid substance.
“The Role of Hypoxia in Apolipoprotein E4-Associated Cognitive Impairment: Implications for Neurodegeneration and Sleep-Disordered Breathing” https://www.ncbi.nlm.nih.gov/pubmed/16335323
Obesity/overfeeding
There are different mechanisms proposed to how fructose affects the regulation of appetite. It doesn’t mean that there is only one correct. It could very well be that all the different mechanisms are at play at the same time. I won’t go into detail listing all the possibilities but you can scan through the papers if you want to know more.
What is clear from the different research papers is that fructose causes increased food intake while glucose has a satiating effect.
“Effects of high-fructose diets on central appetite signaling and cognitive function” https://www.frontiersin.org/articles/10.3389/fnut.2015.00005/full
“Differential effects of central fructose and glucose on hypothalamic malonyl–CoA and food intake” https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2579345/
“Effects of Fructose vs Glucose on Regional Cerebral Blood Flow in Brain Regions Involved With Appetite and Reward Pathways” https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4076145/
“Differential effects of fructose versus glucose on brain and appetitive responses to food cues and decisions for food rewards” https://www.ncbi.nlm.nih.gov/pubmed/25941364
One of the ways obesity is stimulated is by having a high response of insulin which suppresses plasma glucose below baseline resulting in a sense of hunger. Fructose exaggerates the insulin response to glucose so that it will lead to a suppression of glucose below baseline.
“Chronic Fructose Renders Pancreatic β-Cells Hyper-Responsive to Glucose-Stimulated Insulin Secretion Through Extracellular ATP Signaling” https://pubmed.ncbi.nlm.nih.gov/30912960/
Hypertension
How can fructose lead to hypertension? It is clear that animals respond badly to fructose.
Animal studies have shown that high-fructose diets up-regulate sodium and chloride transporters, resulting in a state of salt overload that increases blood pressure. Excess fructose has also been found to activate vasoconstrictors, inactivate vasodilators, and over-stimulate the sympathetic nervous system.
“The mechanisms underlying fructose-induced hypertension: a review” https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4947541/
But not only animals respond bad to it. After reviewing the NHANES data and adjusting for many confounders they found fructose independently associated in US adults without (!!) a history of hypertension. Blood pressure was reviewed in adults who were not diagnosed with hypertension before the study started.
After adjustment for demographics; comorbidities; physical activity; total kilocalorie intake; and dietary confounders such as total carbohydrate, alcohol, salt, and vitamin C intake, an increased fructose intake of ≥74 g/d independently and significantly associated with higher odds of elevated BP levels: It led to a 26, 30, and 77% higher risk for BP cutoffs of ≥135/85, ≥140/90, and ≥160/100 mmHg, respectively. These results suggest that high fructose intake, in the form of added sugar, independently associates with higher BP levels among US adults without a history of hypertension.
“Increased Fructose Associates with Elevated Blood Pressure” https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3013529/
Cholesterol
Also here we see a different effect and again not a good one. I’ll just directly quote from the article abstract.
In contrast, hepatic de novo lipogenesis (DNL) and the 23-hour postprandial triglyceride AUC were increased specifically during fructose consumption. Similarly, markers of altered lipid metabolism and lipoprotein remodeling, including fasting apoB, LDL, small dense LDL, oxidized LDL, and postprandial concentrations of remnant-like particle–triglyceride and –cholesterol significantly increased during fructose but not glucose consumption. In addition, fasting plasma glucose and insulin levels increased and insulin sensitivity decreased in subjects consuming fructose but not in those consuming glucose. These data suggest that dietary fructose specifically increases DNL, promotes dyslipidemia, decreases insulin sensitivity, and increases visceral adiposity in overweight/obese adults.
It shouldn’t be a surprise to see here that insulin sensitivity went down and visceral fat went up. This was covered in the sections above.
So we have an increase in small dense LDL, oxidized LDL and triglycerides. There are communities of researchers who think less of LDL as a marker for atherosclerosis but I think you’ll find almost nobody who doesn’t agree on small dense LDL, (excessively) oxidized LDL and high triglycerides as dangerous markers for increased heart disease.
“Consuming fructose-sweetened, not glucose-sweetened, beverages increases visceral adiposity and lipids and decreases insulin sensitivity in overweight/obese humans” https://www.jci.org/articles/view/37385?ref=binfind.com/web
We see a similar profile in healthy young adults so it is not just an issue of the obese people.
“Consumption of fructose and high fructose corn syrup increase postprandial triglycerides, LDL-cholesterol, and apolipoprotein-B in young men and women.” https://www.ncbi.nlm.nih.gov/pubmed/21849529
Kidney failure
A study on rats shows how the damage builds up with fructose.
Under light microscopy, the kidneys of the HFD group revealed amyloid deposits in Kimmelstiel-Wilson-like nodules and the walls of the large caliber blood vessels, early-stage atherosclerosis with visible ruptures and scarring, hydropic change (vacuolar degeneration) in the epithelial cells covering the proximal tubules, and increased eosinophilia in the distant tubules when compared to the control group.
“Manifestations of Renal Impairment in Fructose-induced Metabolic Syndrome” https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5755946/
One of the causes for kidney failure is the increase in uric acid which is also a cause for kidney stones. The consumption of fructose has a fast response in uric acid production as you can see in the image under (A), the plasma uric acid. The 2 lines at the bottom are the 2 controls.
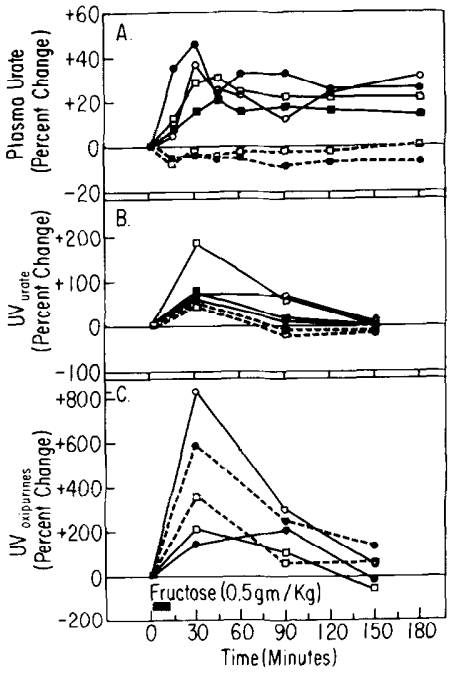
“Studies on the mechanism of fructose-induced hyperuricemia in man” https://www.ncbi.nlm.nih.gov/pubmed/5047915/
“The Epidemiology of Uric Acid and Fructose” https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3197219/
Gout
Another cause of increased uric acid is gout. If fructose increases uric acid then it shouldn’t be a surprise to find that fructose also causes gout.
In a systematic review they found a dose-response relationship between fructose and gout. When you find such a relationship you have a strong indicator of cause and effect.
“Fructose intake and risk of gout and hyperuricemia: a systematic review and meta-analysis of prospective cohort studies” https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5073537/
Cardiovascular Disease
In an experimental setting with rats they developed increased calcification together with all other markers we see in humans including insulin resistance and hyperglycemia.
IR induced by high fructose feeding could evoke osteogenic transdifferentiation of vascular smooth muscle cells (VSMCs) and promote vascular calcification.
“Insulin resistance induces medial artery calcification in fructose-fed rats” https://journals.sagepub.com/doi/abs/10.1258/ebm.2011.011252
Vitamin D
This study is in rats but for now there is no reason to suspect a differential effect in humans. What happens here is that fructose causes a lower serum level of 1,25(OH)2D3. This is the active form of vitamin D. The result is that the serum level of calcium doesn’t increase while it was expected and does take place under glucose instead of fructose feeding.
“Chronic High Fructose Intake Reduces Serum 1,25 (OH)2D3 Levels in Calcium-Sufficient Rodents” https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3981704/
Finally
The volume of papers on the effects of fructose that I referenced above are just a small sample of what you can find. The links with the diseases are strong but is our health policy targeting avoidance of fructose? No.
It is just a guess but I think policy makers and their advisors don’t want fructose to be demonized because it is part of ‘healthy’ fruit.
I don’t want to demonize fruit either. It causes no harm when it is part of a meal or under small amounts such as in berries but I don’t consider fruit necessary.
Necessity
Fruit not necessary? What about the anti-oxidants, vitamines etc.. I hear you ask. Join me for a minute in my imagination where I get dropped in a European wood far from civilization and I have to survive in the vast area, allowed to eat all the fruit I can find.
First of all, I won’t find fruit unless I’m there at the right time of the year. How necessary can it have been in our evolution?
Secondly, when I do find fruit wild in nature, it are berries. Not the monstrous sized apples etc. We cultivated them to be huge. We didn’t go through evolution with access to large fruits, perhaps apart from a few exceptions. At least not in Europe.
Thirdly, when I do succeed to find a source of berries, I’ll be in competition with the rest of the animals who all want to obtain some fructose. They also enjoy the sweet taste.
Fourthly, when I manage to find that source of berries, they are not all ripe at the same time. The 1 or 2 handful that I’ll be able to get the first time will result in about maximum a handful for the next set of days.
If you are lucky you’ll find a berry field at the right time and score some more but the point is that we cannot expect to have evolved on fruit being an important part of our diet because we simply didn’t have access to sufficient quantities for them to make a difference.
Even if it provided us a little edge on survival, today we have no need to build up a fat reserve using fructose to survive winter. Certainly not in the quantities it is consumed today. And we consume a lot through sugar which is half fructose half glucose.
The problem is most apparent when drinking fructose-containing liquids (fruit juice, sugar sweetened beverages).
Sugar
If I can recommend only one thing for people to improve their health then it is to avoid sugar in their diet. The most important to cut out are those fruit juices and sugar sweetened beverages. If you can or as a second phase, cut out sugar entirely from your diet.
You’ll significantly reduce your risk of all the above mentioned diseases.
— THE END —

Leave a comment